
Details of Drug-Drug Interaction
| Drug General Information (ID: DDIXFRZBTH) | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Drug Name | Cyclosporine | Drug Info | Pravastatin | Drug Info | |||||
| Drug Type | Small molecule | Small molecule | |||||||
| Therapeutic Class | Antiviral Agents | Statins/Antihyperlipidemic Agents | |||||||
| Structure | |||||||||
| Mechanism of Cyclosporine-Pravastatin Interaction (Severity Level: Major) | |||||||||
|---|---|---|---|---|---|---|---|---|---|
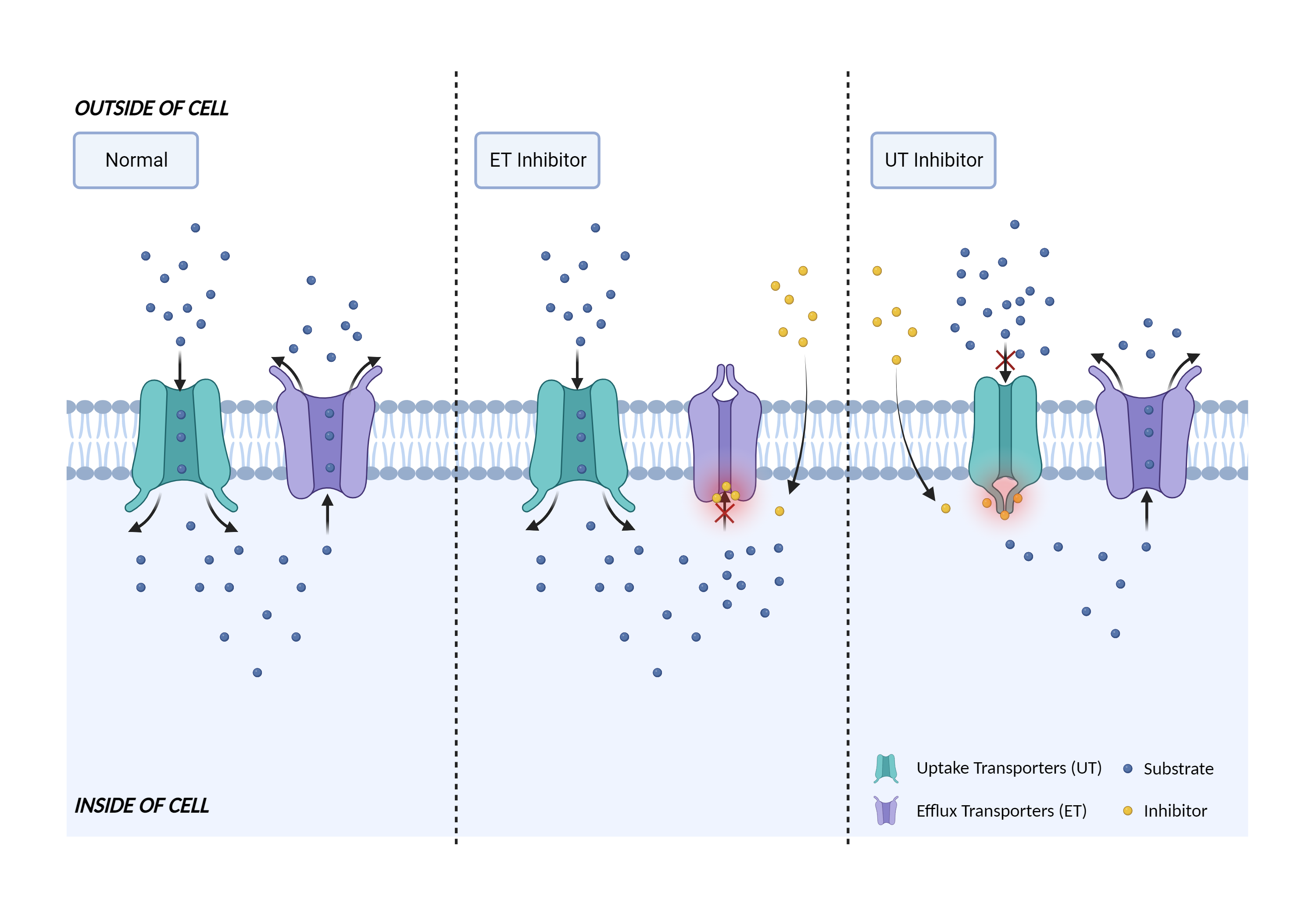
| Transporter inhibition Click to Show/Hide Mechanism Graph | |||||||||
 |
|||||||||
| Drug Name | Cyclosporine | Pravastatin | |||||||
| Mechanism | MRP2 inhibitor | MRP2 substrate | |||||||
| Key Mechanism Factor 1 | |||||||||
| Factor Name | Multidrug resistance-associated protein 2 |
×
Structure
Sequence
MLEKFCNSTFWNSSFLDSPEADLPLCFEQTVLVWIPLGYLWLLAPWQLLHVYKSRTKRSSTTKLYLAKQVFVGFLLILAAIELALVLTEDSGQATVPAVRYTNPSLYLGTWLLVLLIQYSRQWCVQKNSWFLSLFWILSILCGTFQFQTLIRTLLQGDNSNLAYSCLFFISYGFQILILIFSAFSENNESSNNPSSIASFLSSITYSWYDSIILKGYKRPLTLEDVWEVDEEMKTKTLVSKFETHMKRELQKARRALQRRQEKSSQQNSGARLPGLNKNQSQSQDALVLEDVEKKKKKSGTKKDVPKSWLMKALFKTFYMVLLKSFLLKLVNDIFTFVSPQLLKLLISFASDRDTYLWIGYLCAILLFTAALIQSFCLQCYFQLCFKLGVKVRTAIMASVYKKALTLSNLARKEYTVGETVNLMSVDAQKLMDVTNFMHMLWSSVLQIVLSIFFLWRELGPSVLAGVGVMVLVIPINAILSTKSKTIQVKNMKNKDKRLKIMNEILSGIKILKYFAWEPSFRDQVQNLRKKELKNLLAFSQLQCVVIFVFQLTPVLVSVVTFSVYVLVDSNNILDAQKAFTSITLFNILRFPLSMLPMMISSMLQASVSTERLEKYLGGDDLDTSAIRHDCNFDKAMQFSEASFTWEHDSEATVRDVNLDIMAGQLVAVIGPVGSGKSSLISAMLGEMENVHGHITIKGTTAYVPQQSWIQNGTIKDNILFGTEFNEKRYQQVLEACALLPDLEMLPGGDLAEIGEKGINLSGGQKQRISLARATYQNLDIYLLDDPLSAVDAHVGKHIFNKVLGPNGLLKGKTRLLVTHSMHFLPQVDEIVVLGNGTIVEKGSYSALLAKKGEFAKNLKTFLRHTGPEEEATVHDGSEEEDDDYGLISSVEEIPEDAASITMRRENSFRRTLSRSSRSNGRHLKSLRNSLKTRNVNSLKEDEELVKGQKLIKKEFIETGKVKFSIYLEYLQAIGLFSIFFIILAFVMNSVAFIGSNLWLSAWTSDSKIFNSTDYPASQRDMRVGVYGALGLAQGIFVFIAHFWSAFGFVHASNILHKQLLNNILRAPMRFFDTTPTGRIVNRFAGDISTVDDTLPQSLRSWITCFLGIISTLVMICMATPVFTIIVIPLGIIYVSVQMFYVSTSRQLRRLDSVTRSPIYSHFSETVSGLPVIRAFEHQQRFLKHNEVRIDTNQKCVFSWITSNRWLAIRLELVGNLTVFFSALMMVIYRDTLSGDTVGFVLSNALNITQTLNWLVRMTSEIETNIVAVERITEYTKVENEAPWVTDKRPPPDWPSKGKIQFNNYQVRYRPELDLVLRGITCDIGSMEKIGVVGRTGAGKSSLTNCLFRILEAAGGQIIIDGVDIASIGLHDLREKLTIIPQDPILFSGSLRMNLDPFNNYSDEEIWKALELAHLKSFVASLQLGLSHEVTEAGGNLSIGQRQLLCLGRALLRKSKILVLDEATAAVDLETDNLIQTTIQNEFAHCTVITIAHRLHTIMDSDKVMVLDNGKIIECGSPEELLQIPGPFYFMAKEAGIENVNSTKF
|
|||||||
| Gene Name | MRP2 | ||||||||
| Uniprot ID | MRP2_HUMAN | ||||||||
| KEGG Pathway | hsa:1244 | ||||||||
| Protein Family | ABC transporter superfamily | ||||||||
| Protein Function |
ATP-dependent transporter of the ATP-binding cassette (ABC) family that binds and hydrolyzes ATP to enable active transport of various substrates including many drugs, toxicants and endogenous compound across cell membranes. Transports a wide variety of conjugated organic anions such as sulfate-, glucuronide- and glutathione (GSH)-conjugates of endo- and xenobiotics substrates (PubMed:10220572, PubMed:10421658, PubMed:11500505, PubMed:16332456). Mediates hepatobiliary excretion of mono- and bis-glucuronidated bilirubin molecules and therefore play an important role in bilirubin detoxification (PubMed:10421658). Mediates also hepatobiliary excretion of others glucuronide conjugates such as 17beta-estradiol 17-glucosiduronic acid and leukotriene C4 (PubMed:11500505). Transports sulfated bile salt such as taurolithocholate sulfate (PubMed:16332456). Transport various anticancer drugs, such as anthracycline, vinca alkaloid and methotrexate and HIV-drugs such as protease inhibitors (PubMed:10220572, PubMed:11500505, PubMed:12441801). Confers resistance to several anti-cancer drugs including cisplatin, doxorubicin, epirubicin, methotrexate, etoposide and vincristine (PubMed:10220572, PubMed:11500505).
Click to Show/Hide
|
||||||||
| Mechanism Description |
|
||||||||
| Recommended Action | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Management | The benefits of the use of pravastatin in combination with cyclosporine should be carefully weighed against the potential risks. Pravastatin dosage should start at 10 mg/day and generally not exceed 20 mg/day when used in combination with cyclosporine. Higher dosages should be used with caution. All patients treated with HMG-CoA reductase inhibitors should be advised to promptly report any unexplained muscle pain, tenderness, or weakness, particularly if accompanied by malaise or fever. Therapy should be discontinued if creatine kinase is markedly elevated in the absence of strenuous exercise or if myopathy is otherwise suspected or diagnosed. | ||||||||