
Details of Drug-Drug Interaction
| Drug General Information (ID: DDISH8LJD7) | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Drug Name | St. John's Wort | Drug Info | Drospirenone | Drug Info | |||||
| Drug Type | Natural product | Small molecule | |||||||
| Therapeutic Class | Herbal Products/Antidepressants | Contraceptive Agents | |||||||
| Mechanism of St. John's Wort-Drospirenone Interaction (Severity Level: Major) | |||||||||
|---|---|---|---|---|---|---|---|---|---|
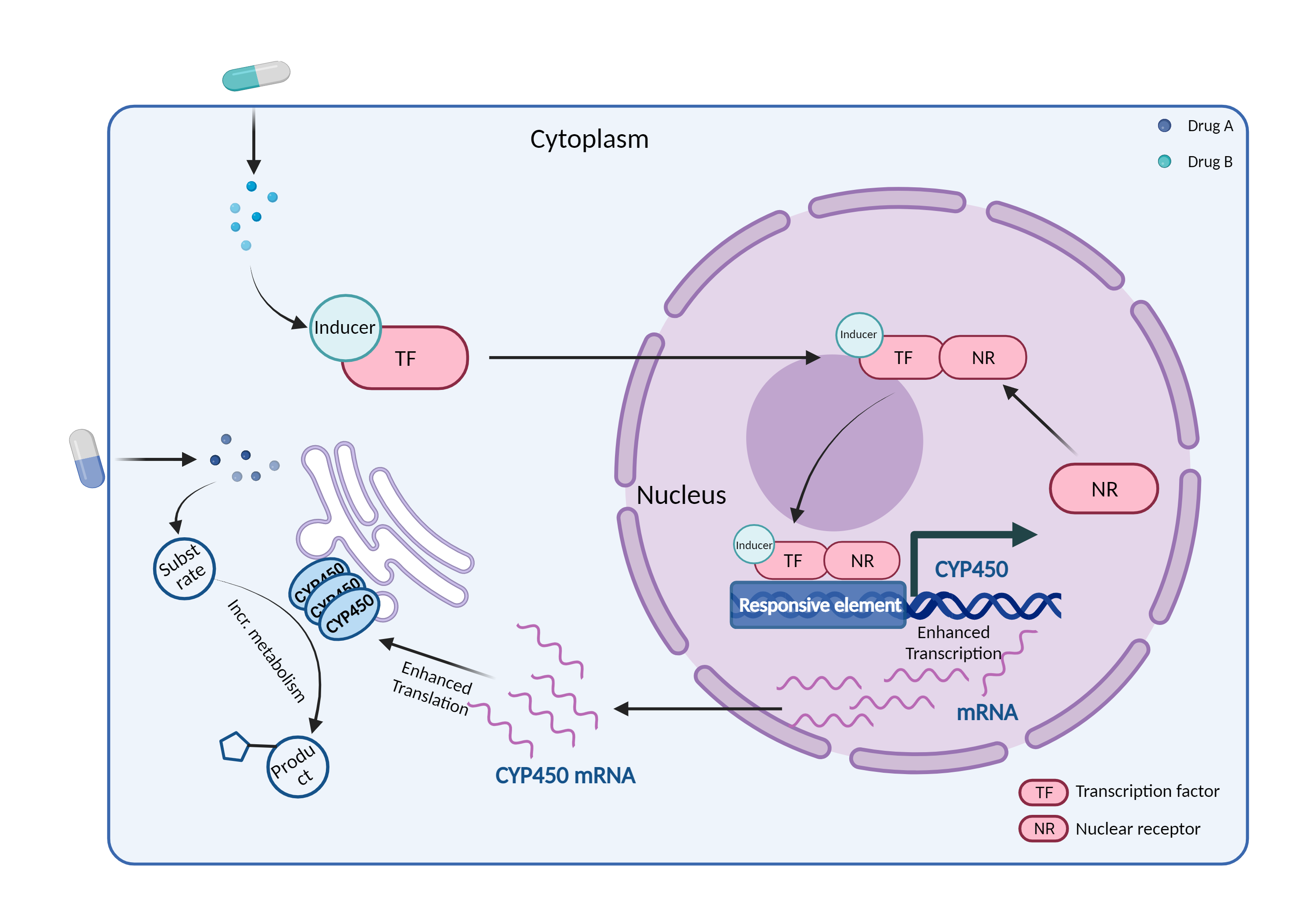
| CYP450 enzyme induction Click to Show/Hide Mechanism Graph | |||||||||
 |
|||||||||
| Drug Name | St. John's Wort | Drospirenone | |||||||
| Mechanism | CYP450 3A4 inducer | CYP450 3A4 substrate | |||||||
| Key Mechanism Factor 1 | |||||||||
| Factor Name | Cytochrome P450 3A4 |
×
Structure
Sequence
MALIPDLAMETWLLLAVSLVLLYLYGTHSHGLFKKLGIPGPTPLPFLGNILSYHKGFCMFDMECHKKYGKVWGFYDGQQPVLAITDPDMIKTVLVKECYSVFTNRRPFGPVGFMKSAISIAEDEEWKRLRSLLSPTFTSGKLKEMVPIIAQYGDVLVRNLRREAETGKPVTLKDVFGAYSMDVITSTSFGVNIDSLNNPQDPFVENTKKLLRFDFLDPFFLSITVFPFLIPILEVLNICVFPREVTNFLRKSVKRMKESRLEDTQKHRVDFLQLMIDSQNSKETESHKALSDLELVAQSIIFIFAGYETTSSVLSFIMYELATHPDVQQKLQEEIDAVLPNKAPPTYDTVLQMEYLDMVVNETLRLFPIAMRLERVCKKDVEINGMFIPKGVVVMIPSYALHRDPKYWTEPEKFLPERFSKKNKDNIDPYIYTPFGSGPRNCIGMRFALMNMKLALIRVLQNFSFKPCKETQIPLKLSLGGLLQPEKPVVLKVESRDGTVSGA
|
|||||||
| Gene Name | CYP3A4 | ||||||||
| Uniprot ID | CP3A4_HUMAN | ||||||||
| KEGG Pathway | hsa:1576 | ||||||||
| Protein Family | Cytochrome P450 family | ||||||||
| Protein Function |
A cytochrome P450 monooxygenase involved in the metabolism of sterols, steroid hormones, retinoids and fatty acids (PubMed:10681376, PubMed:11093772, PubMed:11555828, PubMed:14559847, PubMed:12865317, PubMed:15373842, PubMed:15764715, PubMed:20702771, PubMed:19965576, PubMed:21490593, PubMed:21576599). Mechanistically, uses molecular oxygen inserting one oxygen atom into a substrate, and reducing the second into a water molecule, with two electrons provided by NADPH via cytochrome P450 reductase (NADPH--hemoprotein reductase). Catalyzes the hydroxylation of carbon-hydrogen bonds (PubMed:2732228, PubMed:14559847, PubMed:12865317, PubMed:15373842, PubMed:15764715, PubMed:21576599, PubMed:21490593). Exhibits high catalytic activity for the formation of hydroxyestrogens from estrone (E1) and 17beta-estradiol (E2), namely 2-hydroxy E1 and E2, as well as D-ring hydroxylated E1 and E2 at the C-16 position (PubMed:11555828, PubMed:14559847, PubMed:12865317). Plays a role in the metabolism of androgens, particularly in oxidative deactivation of testosterone (PubMed:2732228, PubMed:15373842, PubMed:15764715, PubMed:22773874). Metabolizes testosterone to less biologically active 2beta- and 6beta-hydroxytestosterones (PubMed:2732228, PubMed:15373842, PubMed:15764715). Contributes to the formation of hydroxycholesterols (oxysterols), particularly A-ring hydroxylated cholesterol at the C-4beta position, and side chain hydroxylated cholesterol at the C-25 position, likely contributing to cholesterol degradation and bile acid biosynthesis (PubMed:21576599). Catalyzes bisallylic hydroxylation of polyunsaturated fatty acids (PUFA) (PubMed:9435160). Catalyzes the epoxidation of double bonds of PUFA with a preference for the last double bond (PubMed:19965576). Metabolizes endocannabinoid arachidonoylethanolamide (anandamide) to 8,9-, 11,12-, and 14,15-epoxyeicosatrienoic acid ethanolamides (EpETrE-EAs), potentially modulating endocannabinoid system signaling (PubMed:20702771). Plays a role in the metabolism of retinoids. Displays high catalytic activity for oxidation of all-trans-retinol to all-trans-retinal, a rate-limiting step for the biosynthesis of all-trans-retinoic acid (atRA) (PubMed:10681376). Further metabolizes atRA toward 4-hydroxyretinoate and may play a role in hepatic atRA clearance (PubMed:11093772). Responsible for oxidative metabolism of xenobiotics. Acts as a 2-exo-monooxygenase for plant lipid 1,8-cineole (eucalyptol) (PubMed:11159812). Metabolizes the majority of the administered drugs. Catalyzes sulfoxidation of the anthelmintics albendazole and fenbendazole (PubMed:10759686). Hydroxylates antimalarial drug quinine (PubMed:8968357). Acts as a 1,4-cineole 2-exo-monooxygenase (PubMed:11695850). Also involved in vitamin D catabolism and calcium homeostasis. Catalyzes the inactivation of the active hormone calcitriol (1-alpha,25-dihydroxyvitamin D(3)) (PubMed:29461981).
Click to Show/Hide
|
||||||||
| Mechanism Description |
|
||||||||
| Recommended Action | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Management | In general, patients should consult a healthcare provider before taking any herbal or alternative medicine. Women using hormonal contraceptives should be advised of the risk of breakthrough bleeding and unintended pregnancy during concomitant therapy with St. John's wort. alternative or additional methods of birth control should be used during and for at least two weeks after short-term and 4 weeks after long-term (greater than 4 weeks) St. John's wort therapy. If a combination oral contraceptive pill is used, a regimen containing at least 50 mcg of ethinyl estradiol per day or equivalent should be selected. Although breakthrough bleeding is not necessarily indicative of low ethinyl estradiol serum levels or increased risk of ovulation, some clinicians suggest that women who experience breakthrough bleeding during enzyme-inducing therapy may be prescribed an increased dose of ethinyl estradiol above 50 mcg daily by combining more than one formulation of contraceptive pill if necessary. For emergency contraception in patients who have used an hepatic enzyme inducer in the past 4 weeks, a non-hormonal emergency contraceptive (e.g., copper intrauterine device) is considered preferable. If this is not possible, some authorities recommend that the usual dose of levonorgestrel (1.5 mg) should be doubled to 3 mg and taken as a single dose as soon as possible (within 72 hours of unprotected sexual intercourse). However, there are no data on efficacy, compliance, or side effects of this regimen. For women with the etonogestrel subdermal implant, the addition of a barrier method is recommended during concomitant use and for 28 days after discontinuation of hepatic enzyme inducing drugs. It is recommended to remove the implant and to prescribe a nonhormonal method in women who require long-term treatment with hepatic enzyme inducing drugs. No precautions or recommendations are available for women using hormone-releasing intrauterine systems, but a significant interaction with these systems is thought to be unlikely due to their local action. Injectable progestin-only contraceptives are also thought to be unaffected by enzyme-inducing drugs. | ||||||||