
Details of Drug-Drug Interaction
| Drug General Information (ID: DDID8QI6HE) | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Drug Name | Minoxidil | Drug Info | Selexipag | Drug Info | |||||
| Drug Type | Small molecule | Small molecule | |||||||
| Therapeutic Class | Antihypertensive Agents | Agents For Pulmonary Hypertension | |||||||
| Structure | |||||||||
| Mechanism of Minoxidil-Selexipag Interaction (Severity Level: Moderate) | |||||||||
|---|---|---|---|---|---|---|---|---|---|
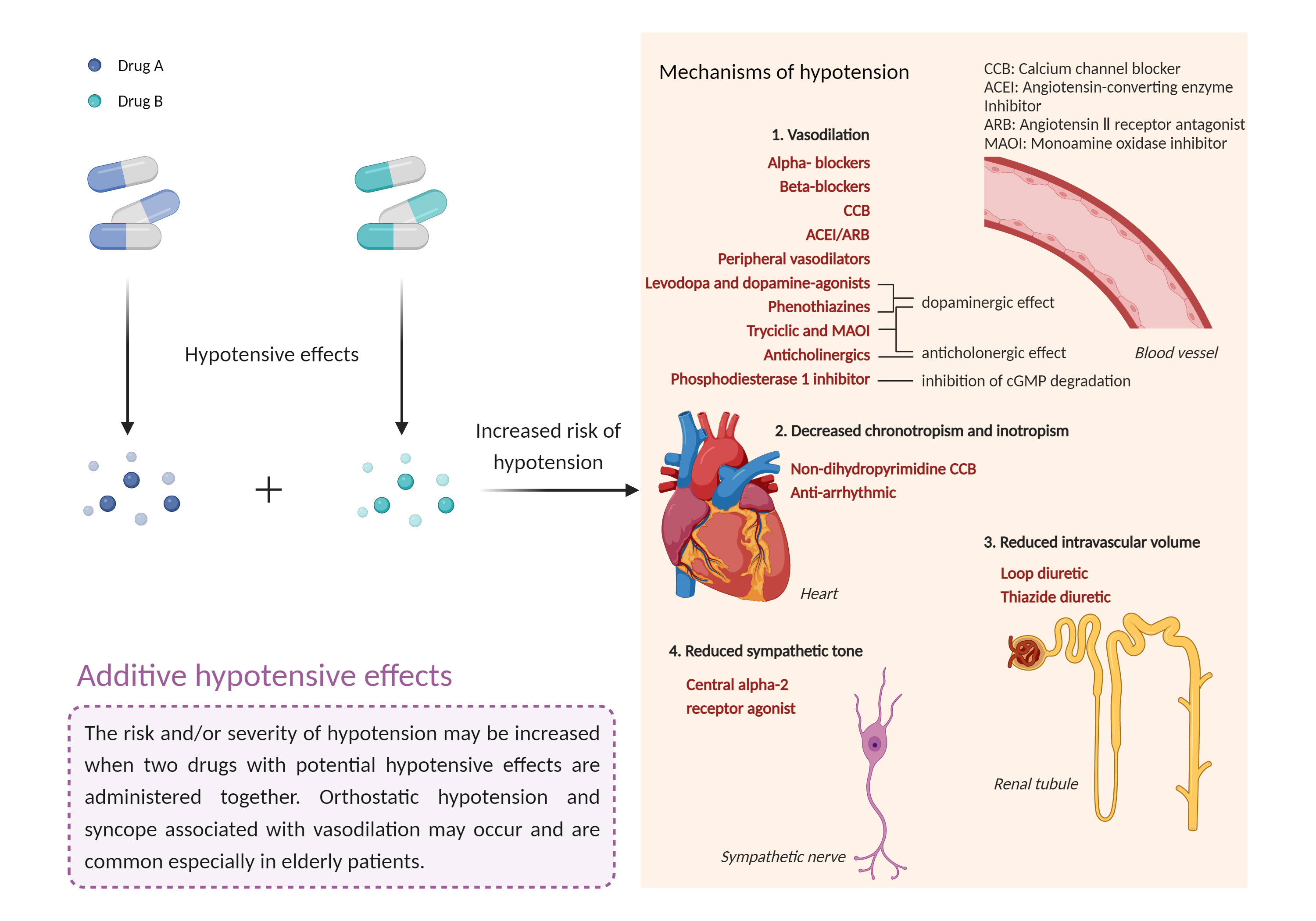
| Additive hypotensive effects Click to Show/Hide Mechanism Graph | |||||||||
 |
|||||||||
| Drug Name | Minoxidil | Selexipag | |||||||
| Mechanism |
Antihypertensive agent ATP-sensitive inward rectifier potassium channel Inducer |
Hypotensive effects Prostacyclin receptor Agonist |
|||||||
| Key Mechanism Factor 1 | |||||||||
| Factor Name | Inward rectifier potassium channel | Structure Sequence | |||||||
| Protein Family | Inward rectifier-type potassium channel (TC 1.A.2.1) family | ||||||||
| Protein Function |
This receptor is controlled by G proteins. Inward rectifier potassium channels are characterized by a greater tendency to allow potassium to flow into the cell rather than out of it. Their voltage dependence is regulated by the concentration of extracellular potassium; as external potassium is raised, the voltage range of the channel opening shifts to more positive voltages. The inward rectification is mainly due to the blockage of outward current by internal magnesium. Can be blocked by extracellular barium (By similarity). Subunit of ATP-sensitive potassium channels (KATP). Can form cardiac and smooth muscle-type KATP channels with ABCC9. KCNJ11 forms the channel pore while ABCC9 is required for activation and regulation.
Click to Show/Hide
|
||||||||
| Key Mechanism Factor 2 | |||||||||
| Factor Name | Prostacyclin receptor |
×
Structure
Sequence
MADSCRNLTYVRGSVGPATSTLMFVAGVVGNGLALGILSARRPARPSAFAVLVTGLAATDLLGTSFLSPAVFVAYARNSSLLGLARGGPALCDAFAFAMTFFGLASMLILFAMAVERCLALSHPYLYAQLDGPRCARLALPAIYAFCVLFCALPLLGLGQHQQYCPGSWCFLRMRWAQPGGAAFSLAYAGLVALLVAAIFLCNGSVTLSLCRMYRQQKRHQGSLGPRPRTGEDEVDHLILLALMTVVMAVCSLPLTIRCFTQAVAPDSSSEMGDLLAFRFYAFNPILDPWVFILFRKAVFQRLKLWVCCLCLGPAHGDSQTPLSQLASGRRDPRAPSAPVGKEGSCVPLSAWGEGQVEPLPPTQQSSGSAVGTSSKAEASVACSLC
|
|||||||
| Gene Name | PTGIR | ||||||||
| Uniprot ID | PI2R_HUMAN | ||||||||
| KEGG Pathway | hsa:5739 | ||||||||
| Protein Family | G-protein coupled receptor 1 family | ||||||||
| Protein Function |
Receptor for prostacyclin (prostaglandin I2 or PGI2). The activity of this receptor is mediated by G(s) proteins which activate adenylate cyclase.
Click to Show/Hide
|
||||||||
| Mechanism Description |
|
||||||||
| Recommended Action | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Management | While therapies that target the prostacyclin pathway have been used in combination with diuretics, antihypertensives, or other vasodilators in the management of pulmonary arterial hypertension, caution is recommended if they must be administered concurrently. If these drugs are used together, it is generally recommended that blood pressure be measured more frequently until a stable blood pressure pattern is observed. Patients should be advised to avoid rising abruptly from a sitting or recumbent position and to notify their doctor if they experience dizziness, lightheadedness, syncope, orthostatic hypotension, or tachycardia. | ||||||||