
Details of Drug-Drug Interaction
| Drug General Information (ID: DDICS2FB1N) | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Drug Name | Rifampicin | Drug Info | Fosamprenavir | Drug Info | |||||
| Drug Type | Small molecule | Small molecule | |||||||
| Therapeutic Class | Antituberculosis Agents | Anti-Hiv Agents | |||||||
| Structure | |||||||||
| Mechanism of Rifampicin-Fosamprenavir Interaction (Severity Level: Major) | |||||||||
|---|---|---|---|---|---|---|---|---|---|
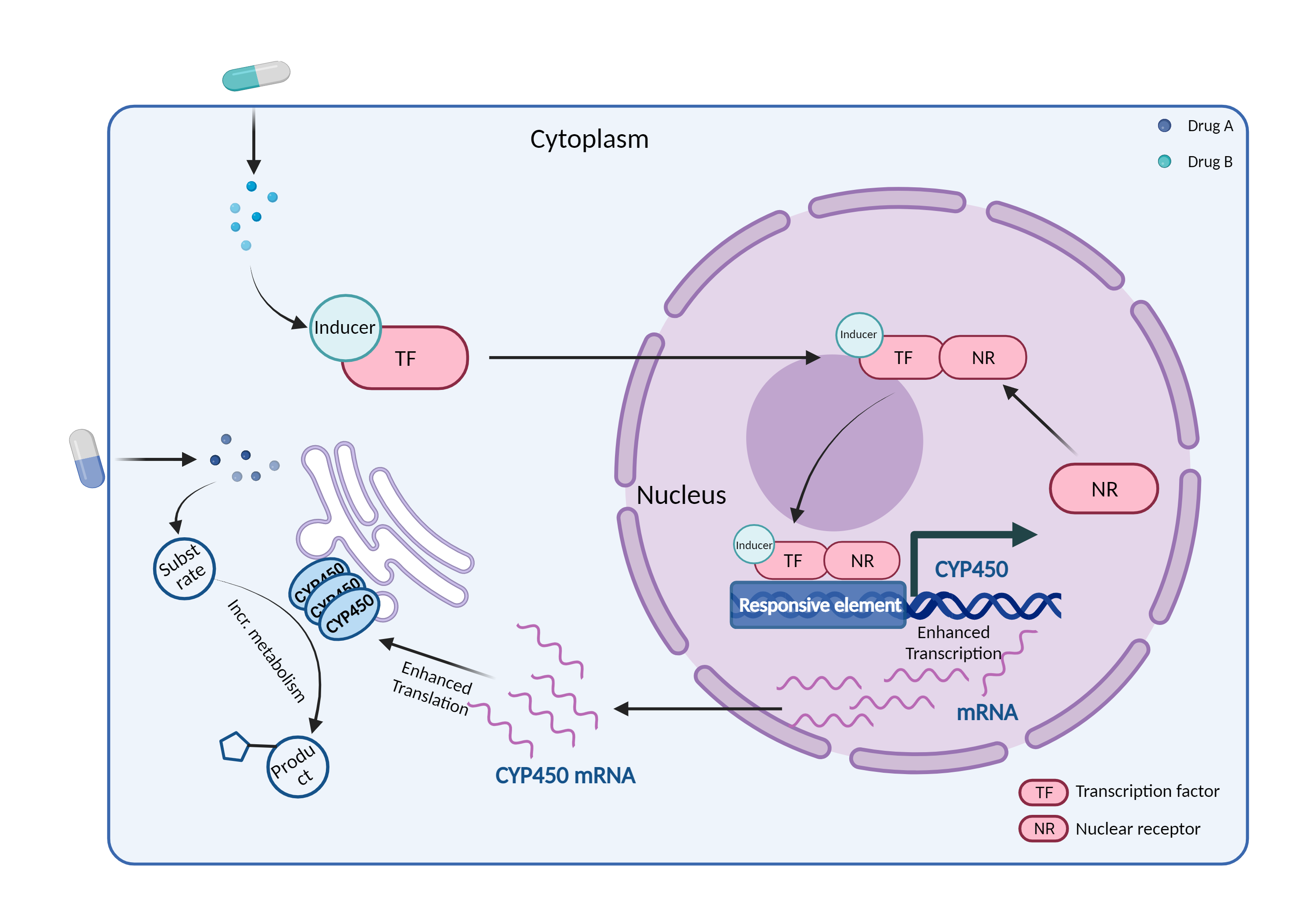
| CYP450 enzyme induction Click to Show/Hide Mechanism Graph | |||||||||
 |
|||||||||
| Drug Name | Rifampicin | Fosamprenavir | |||||||
| Mechanism | CYP450 3A4 inducer | CYP450 3A4 substrate | |||||||
| Key Mechanism Factor 1 | |||||||||
| Factor Name | Cytochrome P450 3A4 |
×
Structure
Sequence
MALIPDLAMETWLLLAVSLVLLYLYGTHSHGLFKKLGIPGPTPLPFLGNILSYHKGFCMFDMECHKKYGKVWGFYDGQQPVLAITDPDMIKTVLVKECYSVFTNRRPFGPVGFMKSAISIAEDEEWKRLRSLLSPTFTSGKLKEMVPIIAQYGDVLVRNLRREAETGKPVTLKDVFGAYSMDVITSTSFGVNIDSLNNPQDPFVENTKKLLRFDFLDPFFLSITVFPFLIPILEVLNICVFPREVTNFLRKSVKRMKESRLEDTQKHRVDFLQLMIDSQNSKETESHKALSDLELVAQSIIFIFAGYETTSSVLSFIMYELATHPDVQQKLQEEIDAVLPNKAPPTYDTVLQMEYLDMVVNETLRLFPIAMRLERVCKKDVEINGMFIPKGVVVMIPSYALHRDPKYWTEPEKFLPERFSKKNKDNIDPYIYTPFGSGPRNCIGMRFALMNMKLALIRVLQNFSFKPCKETQIPLKLSLGGLLQPEKPVVLKVESRDGTVSGA
|
|||||||
| Gene Name | CYP3A4 | ||||||||
| Uniprot ID | CP3A4_HUMAN | ||||||||
| KEGG Pathway | hsa:1576 | ||||||||
| Protein Family | Cytochrome P450 family | ||||||||
| Protein Function |
A cytochrome P450 monooxygenase involved in the metabolism of sterols, steroid hormones, retinoids and fatty acids (PubMed:10681376, PubMed:11093772, PubMed:11555828, PubMed:14559847, PubMed:12865317, PubMed:15373842, PubMed:15764715, PubMed:20702771, PubMed:19965576, PubMed:21490593, PubMed:21576599). Mechanistically, uses molecular oxygen inserting one oxygen atom into a substrate, and reducing the second into a water molecule, with two electrons provided by NADPH via cytochrome P450 reductase (NADPH--hemoprotein reductase). Catalyzes the hydroxylation of carbon-hydrogen bonds (PubMed:2732228, PubMed:14559847, PubMed:12865317, PubMed:15373842, PubMed:15764715, PubMed:21576599, PubMed:21490593). Exhibits high catalytic activity for the formation of hydroxyestrogens from estrone (E1) and 17beta-estradiol (E2), namely 2-hydroxy E1 and E2, as well as D-ring hydroxylated E1 and E2 at the C-16 position (PubMed:11555828, PubMed:14559847, PubMed:12865317). Plays a role in the metabolism of androgens, particularly in oxidative deactivation of testosterone (PubMed:2732228, PubMed:15373842, PubMed:15764715, PubMed:22773874). Metabolizes testosterone to less biologically active 2beta- and 6beta-hydroxytestosterones (PubMed:2732228, PubMed:15373842, PubMed:15764715). Contributes to the formation of hydroxycholesterols (oxysterols), particularly A-ring hydroxylated cholesterol at the C-4beta position, and side chain hydroxylated cholesterol at the C-25 position, likely contributing to cholesterol degradation and bile acid biosynthesis (PubMed:21576599). Catalyzes bisallylic hydroxylation of polyunsaturated fatty acids (PUFA) (PubMed:9435160). Catalyzes the epoxidation of double bonds of PUFA with a preference for the last double bond (PubMed:19965576). Metabolizes endocannabinoid arachidonoylethanolamide (anandamide) to 8,9-, 11,12-, and 14,15-epoxyeicosatrienoic acid ethanolamides (EpETrE-EAs), potentially modulating endocannabinoid system signaling (PubMed:20702771). Plays a role in the metabolism of retinoids. Displays high catalytic activity for oxidation of all-trans-retinol to all-trans-retinal, a rate-limiting step for the biosynthesis of all-trans-retinoic acid (atRA) (PubMed:10681376). Further metabolizes atRA toward 4-hydroxyretinoate and may play a role in hepatic atRA clearance (PubMed:11093772). Responsible for oxidative metabolism of xenobiotics. Acts as a 2-exo-monooxygenase for plant lipid 1,8-cineole (eucalyptol) (PubMed:11159812). Metabolizes the majority of the administered drugs. Catalyzes sulfoxidation of the anthelmintics albendazole and fenbendazole (PubMed:10759686). Hydroxylates antimalarial drug quinine (PubMed:8968357). Acts as a 1,4-cineole 2-exo-monooxygenase (PubMed:11695850). Also involved in vitamin D catabolism and calcium homeostasis. Catalyzes the inactivation of the active hormone calcitriol (1-alpha,25-dihydroxyvitamin D(3)) (PubMed:29461981).
Click to Show/Hide
|
||||||||
| Mechanism Description |
|
||||||||
| Recommended Action | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Management | Given the risk of reduced viral susceptibility and resistance development associated with subtherapeutic antiretroviral drug levels, alternative antimycobacterial agents should be considered in patients already receiving effective PI-containing antiretroviral therapy. For treatment of latent tuberculosis (TB) infection, a nine-month regimen of isoniazid may be considered if feasible. For treatment of HIV-related TB, a regimen that includes rifabutin is generally preferred, as rifabutin appears to be as effective as rifampin but is a much less potent inducer of CYP450 3A4. Nonrifamycin-containing regimens may be suboptimal (higher mortality rates higher rates of treatment failure and relapse increased adverse effects longer treatment duration) and are usually not recommended for HIV-related TB except in patients who are intolerant of rifamycins or infected with a rifamycin-resistant isolate. alternatively, rifampin may be used at usual dosages in patients receiving an antiretroviral regimen that includes ritonavir 600 mg or 400 mg twice a day in combination with another PI at a reduced dosage. In patients who have not begun antiretroviral therapy at the time TB treatment is initiated, clinicians may also consider using rifampin and postponing antiretroviral therapy. With early HIV disease, it may be reasonable to monitor CD4 cell count and postpone antiretroviral therapy until TB treatment is complete, since there is low risk of HIV disease progression or death during this period. However, the optimal time for starting antiretroviral therapy should be individualized based on initial response to TB treatment and occurrence of side effects. In patients with low CD4 cell counts, clinicians may consider delaying antiretroviral therapy until after the first one or two months of TB therapy, as side effects are common during this multi-drug phase of TB treatment and may overlap with those of antiretroviral medications. Moreover, delaying antiretroviral therapy may ameliorate adherence issues and decrease the frequency and severity of paradoxical reactions (i.e., immune restoration syndromes resembling exacerbation of TB that sometimes occur after initiation of antituberculosis treatment in patients receiving potent antiretroviral therapy). Rifabutin can be substituted approximately 2 weeks before the planned initiation of antiretroviral therapy to allow time for rifampin's enzyme induction effects to wane. In general, treatment of TB in the context of antiretroviral therapy is complex and requires an individualized approach. Experts in the treatment of HIV-related tuberculosis should be consulted, and TB and HIV care providers should work in close coordination throughout treatment. | ||||||||