
Details of Drug-Drug Interaction
| Drug General Information (ID: DDIU6F0X8H) | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Drug Name | Imipramine | Drug Info | Propafenone | Drug Info | |||||
| Drug Type | Small molecule | Small molecule | |||||||
| Therapeutic Class | Antidepressants | Antiarrhythmic Agents | |||||||
| Structure | |||||||||
| Mechanism of Imipramine-Propafenone Interaction (Severity Level: Moderate) | |||||||||
|---|---|---|---|---|---|---|---|---|---|
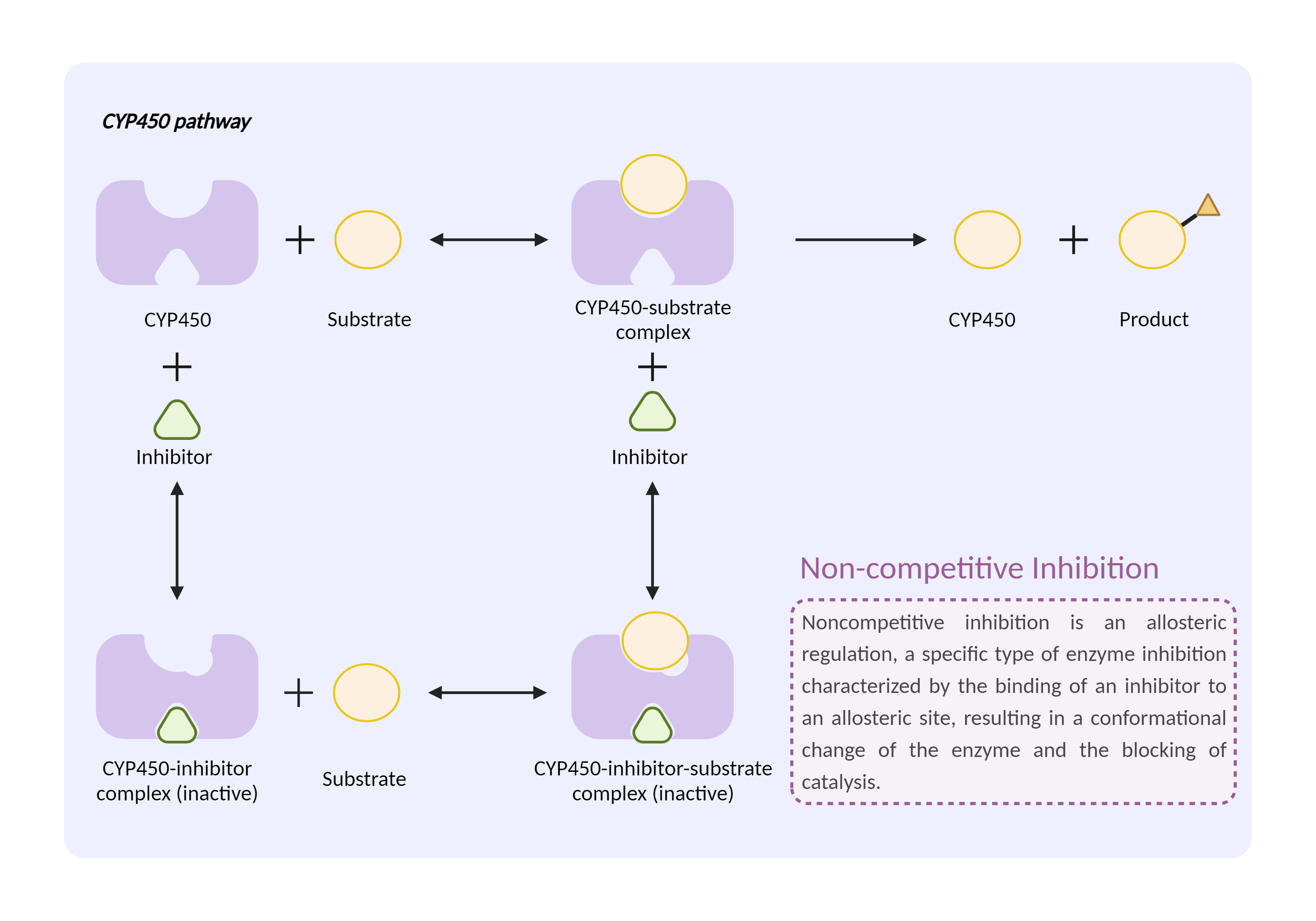
| CYP450 enzyme inhibition Click to Show/Hide Mechanism Graph | |||||||||
 |
|||||||||
| Drug Name | Imipramine | Propafenone | |||||||
| Mechanism 1 | CYP450 2D6 substrate | CYP450 2D6 inhibitor | |||||||
| Key Mechanism Factor 1 | |||||||||
| Factor Name | Cytochrome P450 2D6 |
×
Structure
Sequence
MGLEALVPLAVIVAIFLLLVDLMHRRQRWAARYPPGPLPLPGLGNLLHVDFQNTPYCFDQLRRRFGDVFSLQLAWTPVVVLNGLAAVREALVTHGEDTADRPPVPITQILGFGPRSQGVFLARYGPAWREQRRFSVSTLRNLGLGKKSLEQWVTEEAACLCAAFANHSGRPFRPNGLLDKAVSNVIASLTCGRRFEYDDPRFLRLLDLAQEGLKEESGFLREVLNAVPVLLHIPALAGKVLRFQKAFLTQLDELLTEHRMTWDPAQPPRDLTEAFLAEMEKAKGNPESSFNDENLRIVVADLFSAGMVTTSTTLAWGLLLMILHPDVQRRVQQEIDDVIGQVRRPEMGDQAHMPYTTAVIHEVQRFGDIVPLGVTHMTSRDIEVQGFRIPKGTTLITNLSSVLKDEAVWEKPFRFHPEHFLDAQGHFVKPEAFLPFSAGRRACLGEPLARMELFLFFTSLLQHFSFSVPTGQPRPSHHGVFAFLVSPSPYELCAVPR
|
|||||||
| Gene Name | CYP2D6 | ||||||||
| Uniprot ID | CP2D6_HUMAN | ||||||||
| KEGG Pathway | hsa:1565 | ||||||||
| Protein Family | Cytochrome P450 family | ||||||||
| Protein Function |
A cytochrome P450 monooxygenase involved in the metabolism of fatty acids, steroids and retinoids (PubMed:18698000, PubMed:19965576, PubMed:20972997, PubMed:21289075, PubMed:21576599). Mechanistically, uses molecular oxygen inserting one oxygen atom into a substrate, and reducing the second into a water molecule, with two electrons provided by NADPH via cytochrome P450 reductase (NADPH--hemoprotein reductase) (PubMed:18698000, PubMed:19965576, PubMed:20972997, PubMed:21289075, PubMed:21576599). Catalyzes the epoxidation of double bonds of polyunsaturated fatty acids (PUFA) (PubMed:19965576, PubMed:20972997). Metabolizes endocannabinoid arachidonoylethanolamide (anandamide) to 20-hydroxyeicosatetraenoic acid ethanolamide (20-HETE-EA) and 8,9-, 11,12-, and 14,15-epoxyeicosatrienoic acid ethanolamides (EpETrE-EAs), potentially modulating endocannabinoid system signaling (PubMed:18698000, PubMed:21289075). Catalyzes the hydroxylation of carbon-hydrogen bonds. Metabolizes cholesterol toward 25-hydroxycholesterol, a physiological regulator of cellular cholesterol homeostasis (PubMed:21576599). Catalyzes the oxidative transformations of all-trans retinol to all-trans retinal, a precursor for the active form all-trans-retinoic acid (PubMed:10681376). Also involved in the oxidative metabolism of drugs such as antiarrhythmics, adrenoceptor antagonists, and tricyclic antidepressants.
Click to Show/Hide
|
||||||||
| Mechanism Description |
|
||||||||
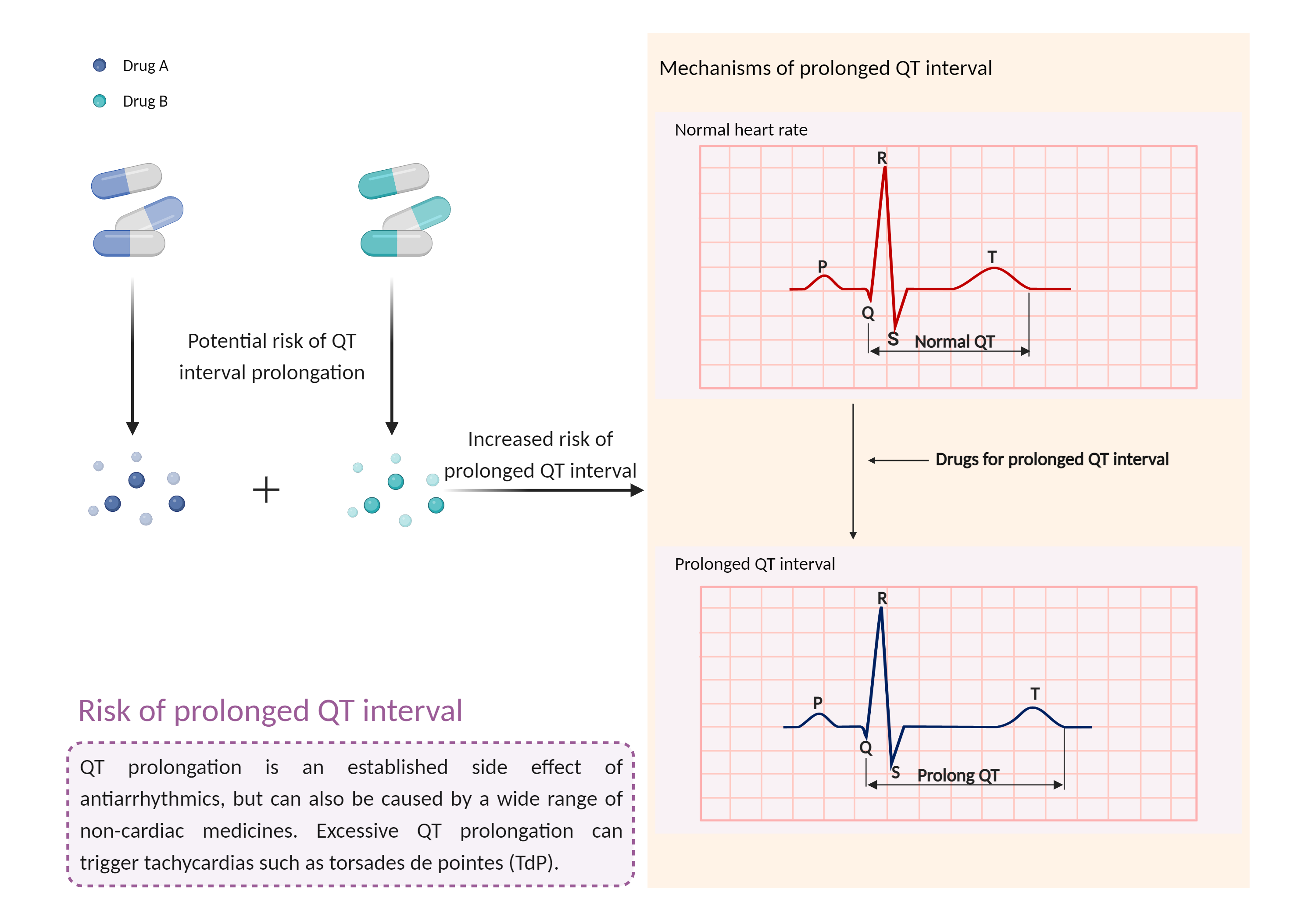
| Increased risk of prolong QT interval Click to Show/Hide Mechanism Graph | |||||||||
 |
|||||||||
| Drug Name | Imipramine | Propafenone | |||||||
| Mechanism 2 | Prolong QT interval | Prolong QT interval | |||||||
| Key Mechanism Factor 2 | |||||||||
| Factor Name | QT interval | ||||||||
| Factor Description | Long QT syndrome is a heart signaling disorder that can cause a fast, chaotic heartbeat (arrhythmia). Many people may not exhibit symptoms, and usually the condition is detected during routine medical tests. In others, the most common symptoms include: sudden fainting, palpitations, dizziness, seizures, sudden death. | ||||||||
| Mechanism Description |
|
||||||||
| Recommended Action | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Management | Caution and clinical monitoring are recommended if a class IC antiarrhythmic agent is prescribed in combination with a tricyclic antidepressant. Pharmacologic response and serum TCA levels should be monitored more closely whenever a class IC antiarrhythmic agent is added to or withdrawn from therapy, and the TCA dosage adjusted as necessary. Patients should be advised to notify their physician if they experience possible signs and symptoms of TCA toxicity such as excessive sedation, dry mouth, blurred vision, urinary retention, constipation, tachycardia, arrhythmia, and seizures. Patients should seek medical attention if they experience symptoms that could indicate the occurrence of torsades de pointes such as dizziness, palpitations, or syncope. | ||||||||