
Details of Drug-Drug Interaction
| Drug General Information (ID: DDITRWZNK4) | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Drug Name | Betaxolol (ophthalmic) | Drug Info | Clonidine | Drug Info | |||||
| Drug Type | Small molecule | Small molecule | |||||||
| Therapeutic Class | Antihypertensive Agents | Antihypertensive Agents | |||||||
| Structure | |||||||||
| Mechanism of Betaxolol (ophthalmic)-Clonidine Interaction (Severity Level: Major) | |||||||||
|---|---|---|---|---|---|---|---|---|---|
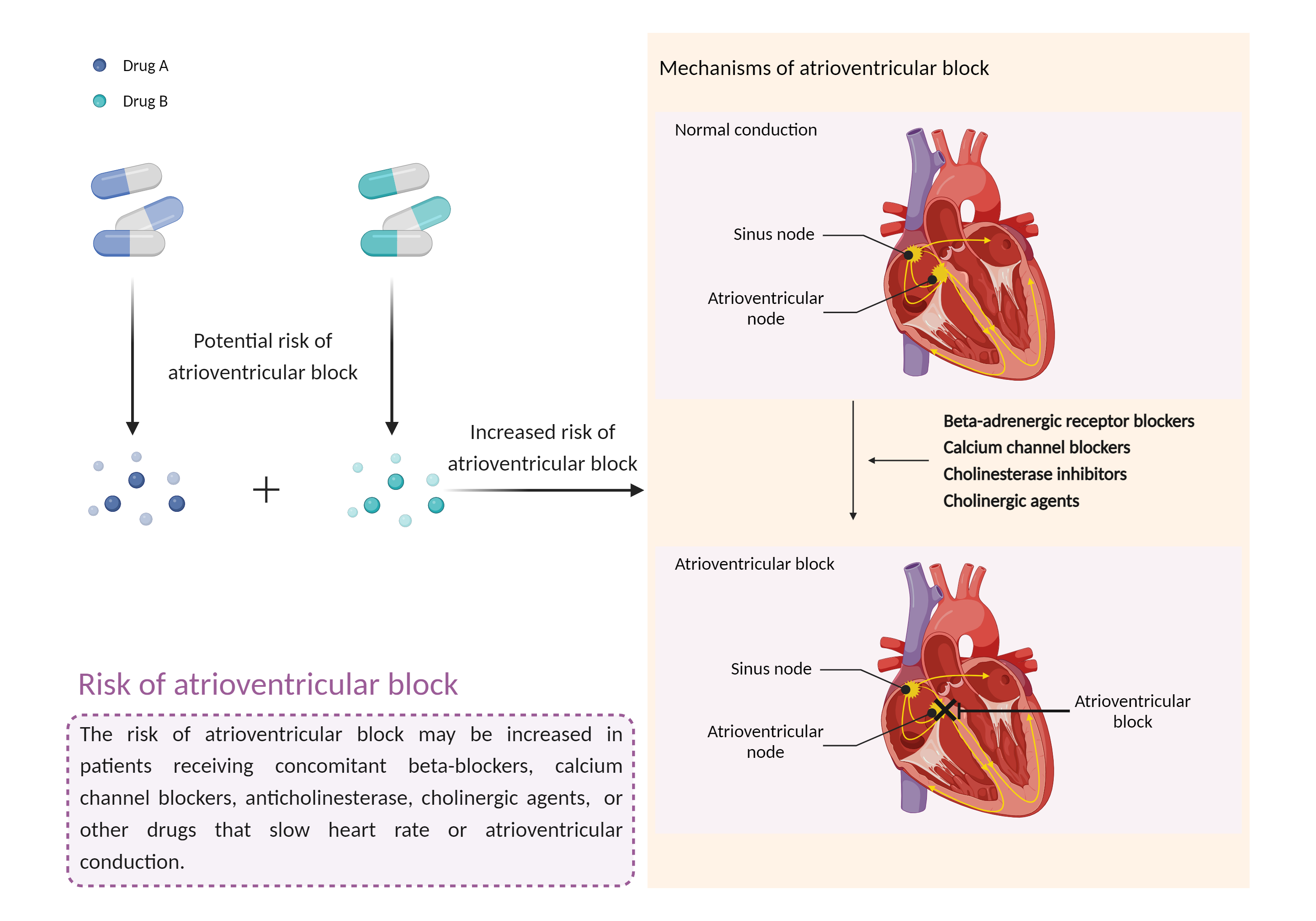
| Increased risk of atrioventricular block Click to Show/Hide Mechanism Graph | |||||||||
 |
|||||||||
| Drug Name | Betaxolol (ophthalmic) | Clonidine | |||||||
| Mechanism 1 | Delay atrioventricular conduction | Delay atrioventricular conduction | |||||||
| Key Mechanism Factor 1 | |||||||||
| Factor Name | Atrioventricular block | ||||||||
| Factor Description | Atrioventricular block is a type of cardiac conduction block that occurs when the electrical signal from the atria to the ventricles is impaired. In an Atrioventricular block, this electrical signal is either delayed or completely blocked. When the signal is completely blocked, the ventricles produce their own electrical signal to control the heart rate. The heart rate produced by the ventricles is much slower than that produced by the sinus node. | ||||||||
| Mechanism Description |
|
||||||||
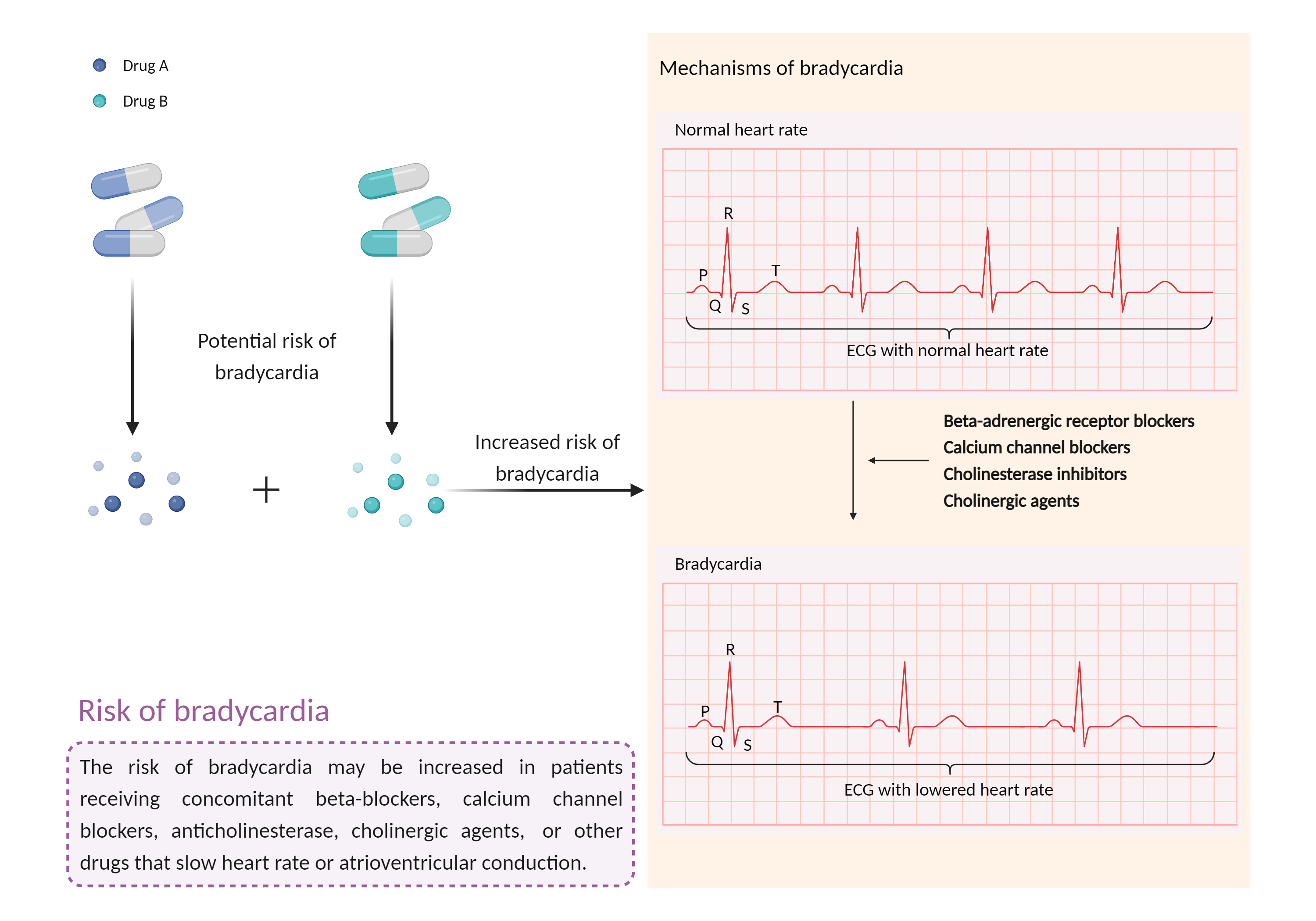
| Increased risk of bradycardia Click to Show/Hide Mechanism Graph | |||||||||
 |
|||||||||
| Drug Name | Betaxolol (ophthalmic) | Clonidine | |||||||
| Mechanism 2 | Bradycardia | Bradycardia | |||||||
| Key Mechanism Factor 2 | |||||||||
| Factor Name | Bradycardia | ||||||||
| Factor Description | Bradycardia is a slow heart rate in which the heart beats less than 60 times per minute. If the heart rate is very slow and the heart is not pumping enough oxygen-rich blood to the body, and you may feel dizzy, very tired or weak, and short of breath. | ||||||||
| Mechanism Description |
|
||||||||
| Recommended Action | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Management | Close monitoring of blood pressure is recommended for patients receiving this combination. Patients should be advised to notify their doctor if they experience a reduced heart rate, dizziness, fainting, or headaches. Clonidine should never be discontinued abruptly, but should be tapered off over 2 to 4 days. The beta blocker should be discontinued a few days before gradually discontinuing the clonidine. It has also been suggested that replacing clonidine and the beta blocker with labetalol (an alpha and beta blocker) may prevent rebound hypertension although some symptoms from increased catecholamine levels occur, or selecting a cardioselective beta blocker (e.g. atenolol, betaxolol, bisoprolol, metoprolol) which is theoretically not expected to exacerbate the pressor response. Patients being withdrawn from clonidine should be carefully monitored for blood pressure changes, severe headache, tremors, apprehension, flushing, nausea, and vomiting. | ||||||||