| Management |
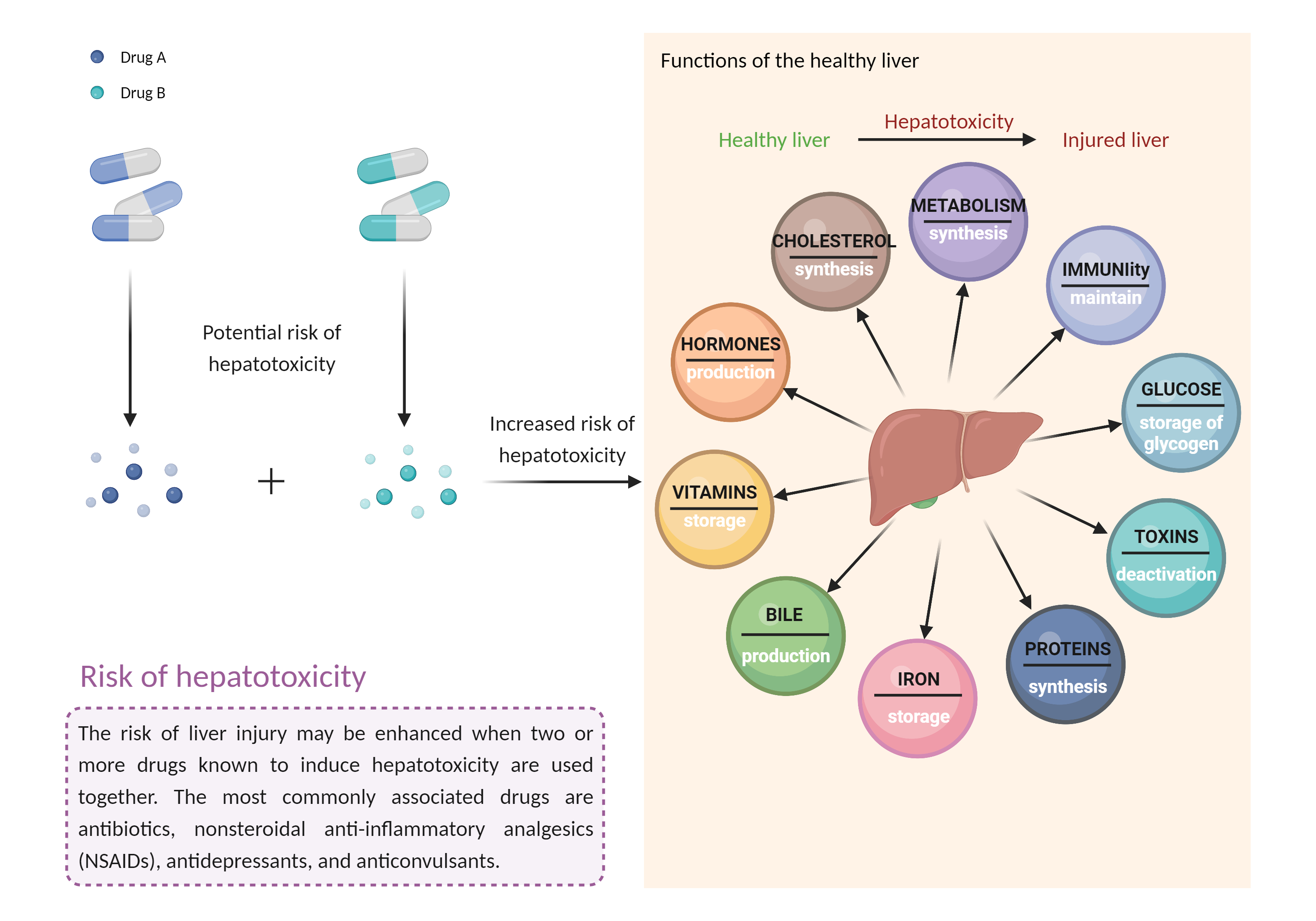
The risk of hepatic injury should be considered when trabectedin is used with other potentially hepatotoxic agents (e.g., acetaminophen alcohol androgens and anabolic steroids antituberculous agents azole antifungal agents ACE inhibitors cyclosporine (high dosages) disulfiram endothelin receptor antagonists interferons ketolide and macrolide antibiotics kinase inhibitors minocycline nonsteroidal anti-inflammatory agents nucleoside reverse transcriptase inhibitors proteasome inhibitors retinoids sulfonamides tamoxifen thiazolidinediones tolvaptan vincristine zileuton anticonvulsants such as carbamazepine, hydantoins, felbamate, and valproic acid lipid-lowering medications such as fenofibrate, lomitapide, mipomersen, niacin, and statins herbals and nutritional supplements such as black cohosh, chaparral, comfrey, DHEA, kava, pennyroyal oil, and red yeast rice). Patients should be advised to seek medical attention if they experience potential signs and symptoms of hepatotoxicity such as fever, rash, itching, anorexia, nausea, vomiting, fatigue, malaise, right upper quadrant pain, dark urine, pale stools, and jaundice. Monitoring of alkaline phosphatase, bilirubin, AST, and ALT should occur regularly during trabectedin treatment in accordance with the product labeling, or as often as necessary when clinical symptoms develop. |