
Details of Drug-Drug Interaction
| Drug General Information (ID: DDIF0H97YK) | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Drug Name | Fluconazole | Drug Info | Fluvastatin | Drug Info | |||||
| Drug Type | Small molecule | Small molecule | |||||||
| Therapeutic Class | Antifungal Agents | Statins/Antihyperlipidemic Agents | |||||||
| Structure | |||||||||
| Mechanism of Fluconazole-Fluvastatin Interaction (Severity Level: Moderate) | |||||||||
|---|---|---|---|---|---|---|---|---|---|
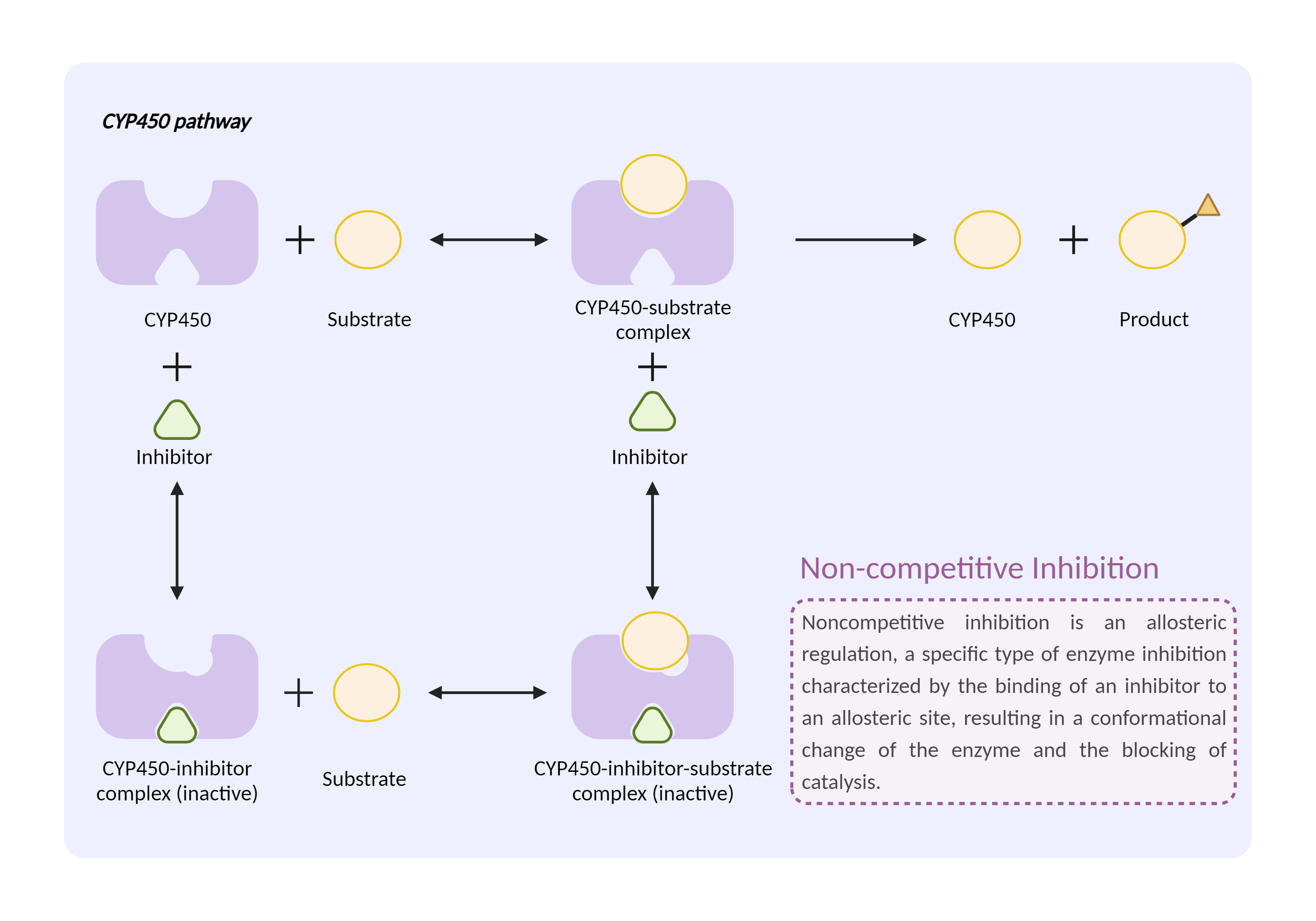
| CYP450 enzyme inhibition Click to Show/Hide Mechanism Graph | |||||||||
 |
|||||||||
| Drug Name | Fluconazole | Fluvastatin | |||||||
| Mechanism | CYP450 2C9 inhibitor | CYP450 2C9 substrate | |||||||
| Key Mechanism Factor 1 | |||||||||
| Factor Name | Cytochrome P450 2C9 |
×
Structure
Sequence
MDSLVVLVLCLSCLLLLSLWRQSSGRGKLPPGPTPLPVIGNILQIGIKDISKSLTNLSKVYGPVFTLYFGLKPIVVLHGYEAVKEALIDLGEEFSGRGIFPLAERANRGFGIVFSNGKKWKEIRRFSLMTLRNFGMGKRSIEDRVQEEARCLVEELRKTKASPCDPTFILGCAPCNVICSIIFHKRFDYKDQQFLNLMEKLNENIKILSSPWIQICNNFSPIIDYFPGTHNKLLKNVAFMKSYILEKVKEHQESMDMNNPQDFIDCFLMKMEKEKHNQPSEFTIESLENTAVDLFGAGTETTSTTLRYALLLLLKHPEVTAKVQEEIERVIGRNRSPCMQDRSHMPYTDAVVHEVQRYIDLLPTSLPHAVTCDIKFRNYLIPKGTTILISLTSVLHDNKEFPNPEMFDPHHFLDEGGNFKKSKYFMPFSAGKRICVGEALAGMELFLFLTSILQNFNLKSLVDPKNLDTTPVVNGFASVPPFYQLCFIPV
|
|||||||
| Gene Name | CYP2C9 | ||||||||
| Uniprot ID | CP2C9_HUMAN | ||||||||
| KEGG Pathway | hsa:1559 | ||||||||
| Protein Family | Cytochrome P450 family | ||||||||
| Protein Function |
A cytochrome P450 monooxygenase involved in the metabolism of various endogenous substrates, including fatty acids and steroids (PubMed:7574697, PubMed:9866708, PubMed:9435160, PubMed:12865317, PubMed:15766564, PubMed:19965576, PubMed:21576599). Mechanistically, uses molecular oxygen inserting one oxygen atom into a substrate, and reducing the second into a water molecule, with two electrons provided by NADPH via cytochrome P450 reductase (NADPH--hemoprotein reductase) (PubMed:7574697, PubMed:9866708, PubMed:9435160, PubMed:12865317, PubMed:15766564, PubMed:19965576, PubMed:21576599). Catalyzes the epoxidation of double bonds of polyunsaturated fatty acids (PUFA) (PubMed:7574697, PubMed:15766564, PubMed:19965576, PubMed:9866708). Catalyzes the hydroxylation of carbon-hydrogen bonds. Metabolizes cholesterol toward 25-hydroxycholesterol, a physiological regulator of cellular cholesterol homeostasis (PubMed:21576599). Exhibits low catalytic activity for the formation of catechol estrogens from 17beta-estradiol (E2) and estrone (E1), namely 2-hydroxy E1 and E2 (PubMed:12865317). Catalyzes bisallylic hydroxylation and hydroxylation with double-bond migration of polyunsaturated fatty acids (PUFA) (PubMed:9866708, PubMed:9435160). Also metabolizes plant monoterpenes such as limonene. Oxygenates (R)- and (S)-limonene to produce carveol and perillyl alcohol (PubMed:11950794). Contributes to the wide pharmacokinetics variability of the metabolism of drugs such as S-warfarin, diclofenac, phenytoin, tolbutamide and losartan (PubMed:25994031).
Click to Show/Hide
|
||||||||
| Mechanism Description |
|
||||||||
| Recommended Action | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Management | Because of the increased risk of musculoskeletal toxicity (e.g., severe myopathy, rhabdomyolysis) associated with high levels of HMG-CoA reductase inhibitory activity in plasma, fluconazole should preferably not be given with fluvastatin. It may be advisable to temporarily discontinue fluvastatin during and for a few days after fluconazole therapy, or consider using another azole antifungal agent such as ketoconazole or itraconazole that is less likely to interfere with CYP450 2C9 metabolism. alternatively, pravastatin has been shown to lack significant interaction with fluconazole and may be a reasonable substitute for fluvastatin. If fluconazole is used with fluvastatin, patients should be closely monitored for early signs and symptoms of myopathy. All patients treated with HMG-CoA reductase inhibitors should be advised to promptly report any unexplained muscle pain, tenderness, or weakness, particularly if accompanied by malaise or fever. Therapy should be discontinued if creatine kinase is markedly elevated in the absence of strenuous exercise or if myopathy is otherwise suspected or diagnosed. | ||||||||