
Details of Drug-Drug Interaction
| Drug General Information (ID: DDI5ECU69Z) | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Drug Name | Carteolol (ophthalmic) | Drug Info | Formoterol | Drug Info | |||||
| Drug Type | Small molecule | Small molecule | |||||||
| Therapeutic Class | Antihypertensive Agents | Sympathomimetics | |||||||
| Structure | |||||||||
| Mechanism of Carteolol (ophthalmic)-Formoterol Interaction (Severity Level: Major) | |||||||||
|---|---|---|---|---|---|---|---|---|---|
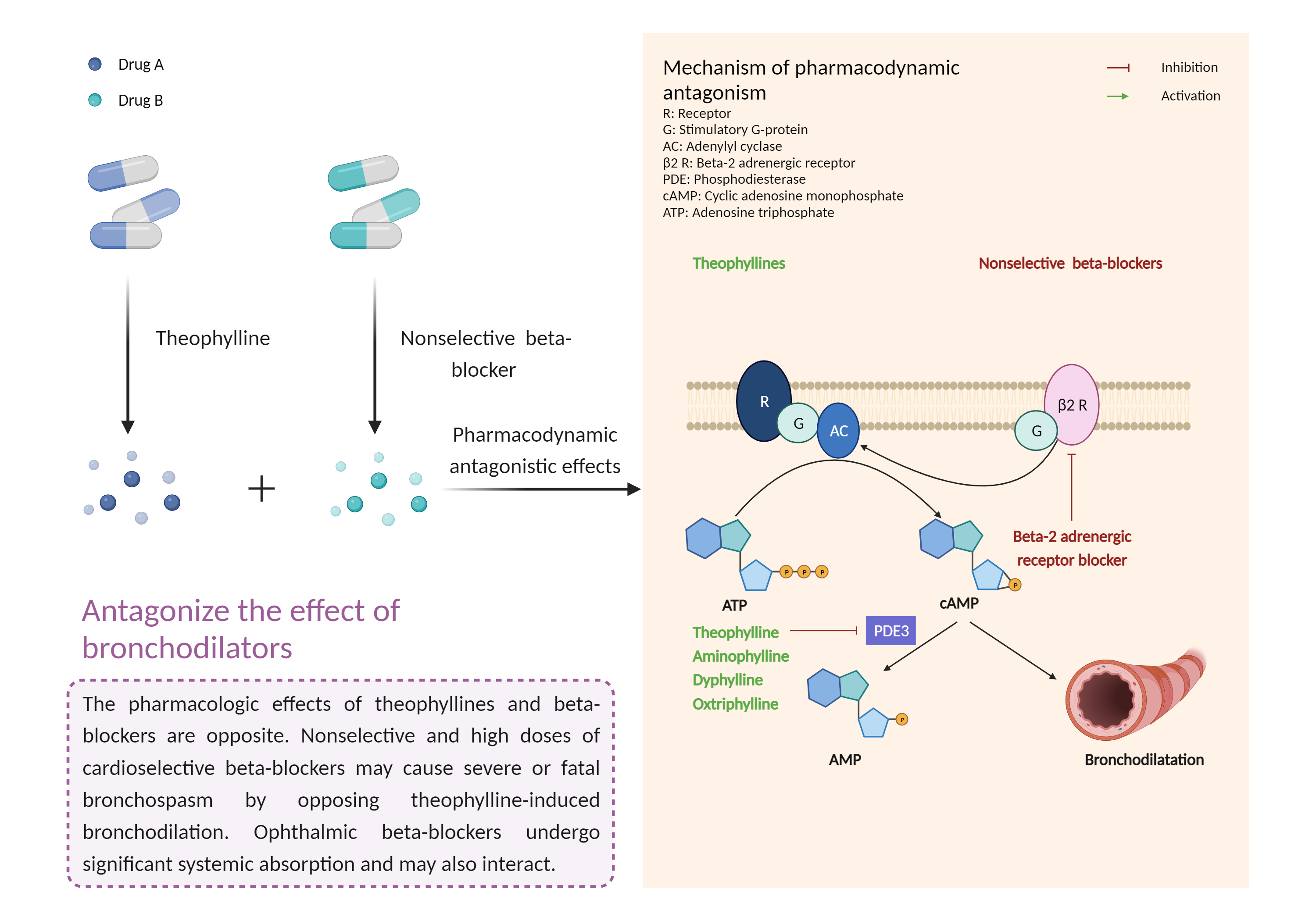
| Antagonize the effect of bronchodilators Click to Show/Hide Mechanism Graph | |||||||||
 |
|||||||||
| Drug Name | Carteolol (ophthalmic) | Formoterol | |||||||
| Mechanism |
Bronchospasm effects Beta-2 adrenergic receptor Antagonist |
Bronchodilator effects Beta-2 adrenergic receptor Agonist |
|||||||
| Key Mechanism Factor 1 | |||||||||
| Factor Name | Adrenergic receptor beta-2 |
×
Structure
Sequence
MGQPGNGSAFLLAPNGSHAPDHDVTQERDEVWVVGMGIVMSLIVLAIVFGNVLVITAIAKFERLQTVTNYFITSLACADLVMGLAVVPFGAAHILMKMWTFGNFWCEFWTSIDVLCVTASIETLCVIAVDRYFAITSPFKYQSLLTKNKARVIILMVWIVSGLTSFLPIQMHWYRATHQEAINCYANETCCDFFTNQAYAIASSIVSFYVPLVIMVFVYSRVFQEAKRQLQKIDKSEGRFHVQNLSQVEQDGRTGHGLRRSSKFCLKEHKALKTLGIIMGTFTLCWLPFFIVNIVHVIQDNLIRKEVYILLNWIGYVNSGFNPLIYCRSPDFRIAFQELLCLRRSSLKAYGNGYSSNGNTGEQSGYHVEQEKENKLLCEDLPGTEDFVGHQGTVPSDNIDSQGRNCSTNDSLL
|
|||||||
| Gene Name | ADRB2 | ||||||||
| Uniprot ID | ADRB2_HUMAN | ||||||||
| KEGG Pathway | hsa:154 | ||||||||
| Protein Family | G-protein coupled receptor 1 family | ||||||||
| Protein Function |
Beta-adrenergic receptors mediate the catecholamine-induced activation of adenylate cyclase through the action of G proteins. The beta-2-adrenergic receptor binds epinephrine with an approximately 30-fold greater affinity than it does norepinephrine.
Click to Show/Hide
|
||||||||
| Mechanism Description |
|
||||||||
| Recommended Action | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Management | Concomitant use of beta-2 adrenergic bronchodilators with beta-blockers, including ophthalmic formulations, should generally be avoided. If coadministration is required, a cardioselective beta-blocker (e.g., acebutolol, atenolol, betaxolol, bisoprolol, metoprolol, nebivolol) is usually preferred. Nevertheless, caution is advised and respiratory status should be closely monitored, as cardioselectivity is not absolute and larger doses of beta-1 selective agents may pose some of the same risks as nonselective agents. In general, nonselective beta-blockers are considered contraindicated in patients with obstructive airways disease. | ||||||||